
Question
Is prenatal exposure to cannabis associated with child outcomes?
Findings
This cross-sectional analysis of 11 489 children (655 exposed to cannabis prenatally) found that prenatal cannabis exposure after maternal knowledge of pregnancy was associated with greater psychopathology during middle childhood, even after accounting for potentially confounding variables.
Meaning
Prenatal cannabis exposure may increase risk for psychopathology; consistent with recent recommendations by the Surgeon General of the United States, these data suggest that cannabis use during pregnancy should be discouraged by clinicians and dispensaries.
Abstract
Importance
In light of increasing cannabis use among pregnant women, the US Surgeon General recently issued an advisory against the use of marijuana during pregnancy.
Objective
To evaluate whether cannabis use during pregnancy is associated with adverse outcomes among offspring.
Design, Setting, and Participants
In this cross-sectional study, data were obtained from the baseline session of the ongoing longitudinal Adolescent Brain and Cognitive Development Study, which recruited 11 875 children aged 9 to 11 years, as well as a parent or caregiver, from 22 sites across the United States between June 1, 2016, and October 15, 2018.
Exposure
Prenatal cannabis exposure prior to and after maternal knowledge of pregnancy.
Main Outcomes and Measures
Symptoms of psychopathology in children (ie, psychotic-like experiences [PLEs] and internalizing, externalizing, attention, thought, and social problems), cognition, sleep, birth weight, gestational age at birth, body mass index, and brain structure (ie, total intracranial volume, white matter volume, and gray matter volume). Covariates included familial (eg, income and familial psychopathology), pregnancy (eg, prenatal exposure to alcohol and tobacco), and child (eg, substance use) variables.
Results
Among 11 489 children (5997 boys [52.2%]; mean [SD] age, 9.9 [0.6] years) with nonmissing prenatal cannabis exposure data, 655 (5.7%) were exposed to cannabis prenatally. Relative to no exposure, cannabis exposure only before (413 [3.6%]) and after (242 [2.1%]) maternal knowledge of pregnancy were associated with greater offspring psychopathology characteristics (ie, PLEs and internalizing, externalizing, attention, thought and, social problems), sleep problems, and body mass index, as well as lower cognition and gray matter volume (all |β| > 0.02; all false discovery rate [FDR]–corrected P < .03). Only exposure after knowledge of pregnancy was associated with lower birth weight as well as total intracranial volume and white matter volumes relative to no exposure and exposure only before knowledge (all |β| > 0.02; all FDR-corrected P < .04). When including potentially confounding covariates, exposure after maternal knowledge of pregnancy remained associated with greater PLEs and externalizing, attention, thought, and social problems (all β > 0.02; FDR-corrected P < .02). Exposure only prior to maternal knowledge of pregnancy did not differ from no exposure on any outcomes when considering potentially confounding variables (all |β| < 0.02; FDR-corrected P > .70).
Conclusions and Relevance
This study suggests that prenatal cannabis exposure and its correlated factors are associated with greater risk for psychopathology during middle childhood. Cannabis use during pregnancy should be discouraged.
Introduction
Alongside increasingly permissive sociocultural attitudes and laws surrounding cannabis,1 past-month cannabis use among pregnant US women increased by 106% from 2002 (3.4%) to 2017 (7.0%).2 Tetrahydrocannabinol (THC), the psychoactive component of cannabis, crosses the placenta and interfaces with the endocannabinoid system, which is associated with neural development.3,4,5 Thus, it is plausible that cannabis use during pregnancy may relate to outcomes in offspring. The increase of cannabis use among pregnant mothers,2,6,7,8 as well as evidence linking prenatal exposure to adverse outcomes,9,10,11,12,13 prompted the US Surgeon General to release an advisory against cannabis use during pregnancy and breastfeeding on August 29, 2019.14
To our knowledge, there have been relatively few investigations of prenatal cannabis exposure and child outcomes. Available evidence has linked exposure to reduced birth weight15 and cognition,16,17 as well as heightened risk for premature birth,18 psychopathology (ie, psychosis, internalizing, and externalizing),19,20,21 and sleep problems.22 However, limited cross-study replication23,24,25 and an inability to account for potential confounders (eg, child substance use and familial risk) in most studies has left these associations tenuous. Indeed, the National Academies of Sciences, Engineering, and Medicine recently concluded that only reduced birth weight has been robustly linked to prenatal cannabis exposure.13
Using data from the Adolescent Brain Cognitive Development (ABCD) Study (data release 2.0.1) of 11 875 children, we test whether prenatal cannabis exposure before and after maternal knowledge of pregnancy is associated with psychopathology (ie, internalizing, externalizing, attention, thought, and social problems, as well as psychotic-like experiences [PLEs]), sleep, cognition, birth weight, premature birth, body mass index (BMI), and gross brain structure (ie, white matter volume [WMV], gray matter volume [GMV], and intracranial volume [ICV]). This study represents a comprehensive extension of a prior investigation of prenatal cannabis exposure and PLEs among the initial ABCD Study data release (N = 4361).26 Cannabis use during the lifetime is associated with various psychosocial and familial correlates.1 In addition, from a neurodevelopmental perspective, endocannabinoid receptors are not expressed in the fetus until 5 to 6 weeks’ gestation,9,27,28 which approximately corresponds to when, in this study, mothers learned they were pregnant (mean [SD], 6.9 [6.8] weeks). Thus, we hypothesized that any observed associations with cannabis exposure only before maternal knowledge of pregnancy would be dependent on potential confounders (eg, socioeconomic status and familial history of psychopathology). However, we expected that associations with maternal use of cannabis after knowledge of pregnancy would partially capture cannabis-specific associations and therefore persist even on inclusion of potentially confounding covariates.
Methods
Participants
Data for this cross-sectional study were collected between June 1, 2016, and October 15, 2018, from children born between 2005 and 2009 to 9987 mothers through 10 801 pregnancies, who completed the baseline session of the ongoing longitudinal ABCD Study (release 2.0.1; https://abcdstudy.org/).29 The study includes a family-based design in which twin (n = 2108), triplet (n = 30), nontwin siblings (n = 1589), and singletons (n = 8148) were recruited. All parents or caregivers (10 131 of 11 875 biological mothers [85.3%]) provided written informed consent and children provided verbal assent to a research protocol approved by the institutional review board at each data collection site (n = 22) throughout the United States (https://abcdstudy.org/sites/abcd-sites.html). All analyses were rerun excluding parent or caregiver respondents who were not the mother; all results and conclusions remained the same; eTable 12 in the Supplement. For our analyses, participants with non-missing prenatal cannabis exposure data were included (n = 11 489; Table 1). This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
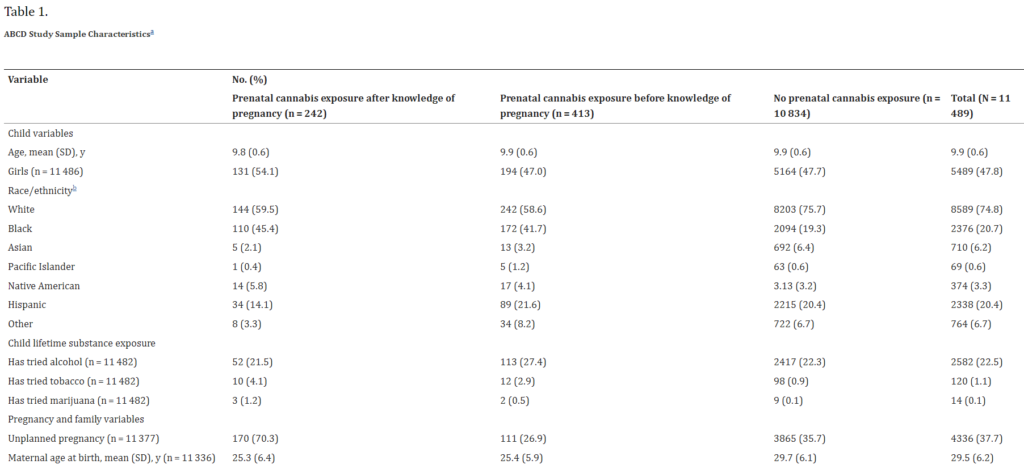
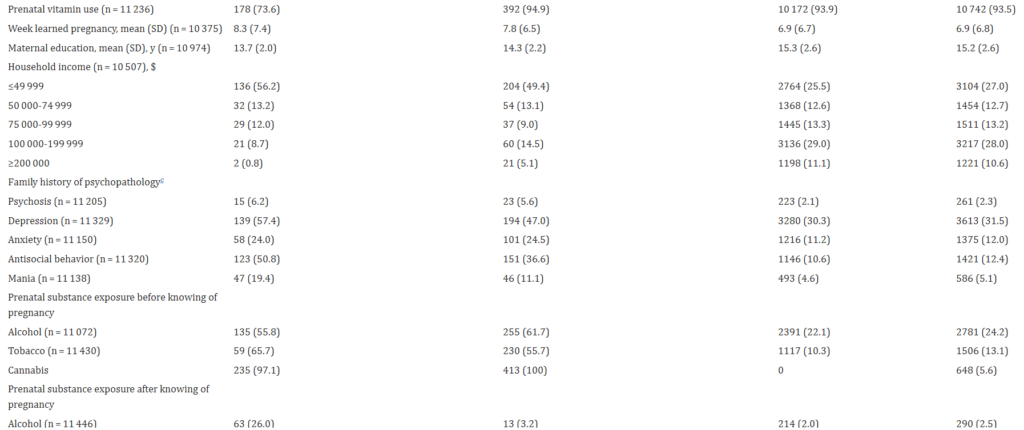
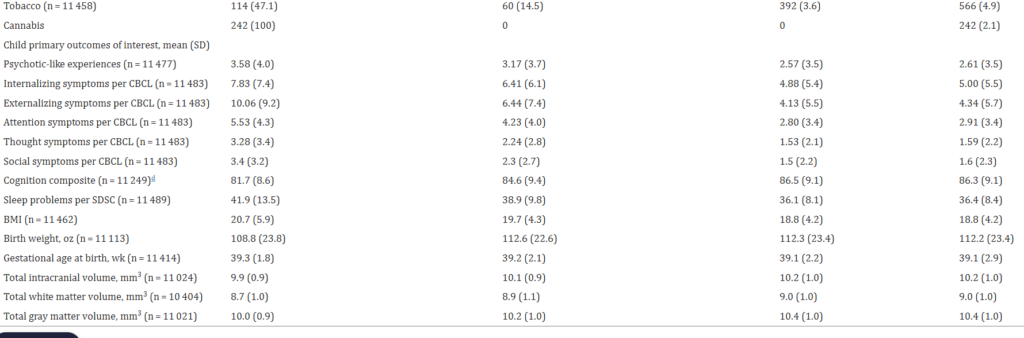
Abbreviations: ABCD, Adolescent Brain and Cognitive Development; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); CBCL, Child Behavior Checklist; SDSC, Parent Sleep Disturbance Scale for Children.
aData included in analyses were required to have a response of yes or no for maternal report of using cannabis prior to and after knowledge of pregnancy. All variables reflect measures assessed during the baseline session when children were a mean (SD) age of 9.9 (0.6) years. In our analytic approach, all but 7 children who were exposed to cannabis prior to maternal knowledge of pregnancy were also coded as having prenatal exposure prior to maternal knowledge. The estimates reported above refer to the nonwinsorized versions of each variable (refer to the eMethods in the Supplement for descriptive information of the winsorized data). Brain metrics were scaled by dividing each value by the SD.bRace/ethnicity variables were coded as non–mutually exclusive dichotomous variables; as such, these numbers do not sum to 100% as participants could be included in multiple categories. cFamily history of depression, psychosis, mania, antisocial behavior, and anxiety among first-degree relatives. Psychotic-like experiences were measured by the Prodromal Questionnaire–Brief Child Version total score. dCognition composite was assessed using the National Institutes of Health Toolbox.
Measures
All measures are described in the eMethods in the Supplement and Table 1. Child prenatal cannabis exposure was based on parent or caregiver retrospective report. Three mutually exclusive groups were formed: no exposure (n = 10 834), exposure prior to maternal knowledge of pregnancy only (n = 413), and exposure after maternal knowledge of pregnancy (n = 242, with or without exposure prior to maternal knowledge).
The Prodromal Questionnaire–Brief Child Version30,31 total score was used to assess child-reported PLEs. Higher scores indicate more PLEs.
The Child Behavior Checklist32 was used to assess broad-spectrum internalizing and externalizing problems as well as attention, thought, and social problems in children according to parent or caregiver report. Higher scores are reflective of more problems.
The National Institutes of Health Toolbox Cognition Battery–Total Cognition Composite33 indexed child cognitive ability. Higher scores indicate greater cognitive performance.
The Sleep Disturbance Scale for Children34 total score was used to assess sleep problems in children according to parent or caregiver report. Higher scores reflect more sleep problems.
A parent or caregiver retrospectively reported their child’s gestational age at birth and birth weight. Child BMI was calculated using measured height and weight.
FreeSurfer, version 5.335 was used to estimate total ICV, GMV, and WMV. See the eMethods in the Supplement for imaging acquisition and processing.36,37,38,39
Covariates
The following fixed-effect covariates were dummy coded: race/ethnicity (White, Black, Asian, Native American, Pacific Islander, Hispanic, and other), first-degree familial history of psychopathology (depression, psychosis, anxiety, mania, and antisocial behavior), prenatal exposure to tobacco or alcohol before or after maternal knowledge of pregnancy, unplanned pregnancy, prenatal vitamin use, child had tried alcohol, child had tried tobacco, child sex, and twin or triplet status. Annual household income was treated as a 5-level categorical variable. The following continuous covariates were included: birth weight, maternal age at birth, gestational age when pregnancy was discovered (weeks), child age, and maternal educational level. These variables were reported by caregivers. Intracranial volume was further included as a covariate in models with GMV and WMV as outcomes. Polygenic scores (PGS) for schizophrenia, educational attainment, and cannabis use as well as ancestrally informative principal components (n = 10) were included as covariates in post hoc analyses within the genomically confirmed European ancestry subsample (eMethods in the Supplement). Owing to limited endorsement of ever having a marijuana puff among children (n = 14), we did not include this variable as a covariate.
Uncommon substance use among children (ie, use other than trying alcohol or tobacco [eg, having a marijuana puff or a full alcoholic drink]) or by women while they were pregnant as well as extreme premature birth (ie, <32 weeks) and nonbiological mother caregiver report were not included as covariates. Post hoc analyses excluded individuals based on these variables (eMethods in the Supplement).
Statistical Analysis
Individual values on continuous predictor and outcome variables were winsorized (to 3 SD) to minimize the influence of extreme values. We used linear mixed-effects models with random intercept parameters to account for site and family membership for all analyses with the lme4 package in R, version 3.6.0 (R Project for Statistical Computing).40 We examined the association between prenatal cannabis exposure and outcomes using 3 analytic approaches.
First, we tested whether mutually exclusive prenatal cannabis exposure groups were associated with outcomes of interest in nested mixed models with no fixed-effect covariates with the following orthogonal contrasts: (1) exposure after maternal knowledge of pregnancy vs no exposure, (2) exposure only before maternal knowledge of pregnancy vs no exposure, and (3) exposure after vs only before maternal knowledge of pregnancy. Benjamini-Hochberg false discovery rate (FDR) correction was used to adjust for testing multiple phenotypes within each group contrast (14 tests). Second, we examined whether any associations that were significant after multiple testing correction were robust to the inclusion of potentially confounding covariates (equations are illustrated in the eMethods in the Supplement), using FDR correction to adjust for multiple testing within each group contrast (13 tests). Third, to account for possible confounding associations of genomic liability with offspring outcomes not accounted for by familial history, we examined associations when accounting for child PGS for related outcomes (eMethods in the Supplement).41 To ensure that effect-size changes could not be attributed to reduced sample size alone, we first recomputed covariate-adjusted associations in the genomically confirmed European ancestry subsample (n = 4591). We then tested whether any significant estimates (P < .05 for any contrast) were altered by inclusion of PGS (ie, schizophrenia,42 educational level,43 and cannabis use44 for PLEs; and cannabis use for social problems; eMethods in the Supplement). Post hoc sensitivity analyses of nonmutually exclusive dummy variables entered into regressions simultaneously and inverse probability propensity score weighting were used to test whether observed associations were robust to analytic alternatives to our mutually exclusive group approach and use of covariates, respectively (eMethods in the Supplement). All P values were from 2-sided tests and results were deemed statistically significant at FDR-corrected P < .05.
Results
Among 11 489 children (5997 boys [52.2%]; mean [SD] age, 9.9 [0.6] years; 8589 of 11 489 White [74.8%]), 655 (5.7%) were prenatally exposed to cannabis (Table 1). Of these, 413 were exposed only before maternal knowledge of pregnancy, 235 were exposed both before and after maternal knowledge, and 7 were exposed only after maternal knowledge. Mothers learned of their pregnancy at a mean (SD) of 6.9 (6.8) weeks. Rates of tobacco and alcohol use during pregnancy were higher than cannabis use and were modestly correlated with prenatal cannabis exposure (tobacco, 1519 of 11 489 [13.2%]; r = 0.34; and alcohol, 2820 of 11 489 [24.5%]; r = 0.20). Data on frequency of cannabis use during pregnancy were collected; however, high rates of missingness (eg, 20%-38%) and nonspecific item wording (“how many times per day”) preclude meaningful analyses. Of those with reported data, 87.0% of those in the exposure only before maternal knowledge group (287 of 330) and 92.7% of those in the exposure after maternal knowledge group (140 of 151) reported using cannabis at least once per day; groups did not differ in reported frequency of use during pregnancy (t = 0.43; P = .67).
Prenatal Cannabis Exposure and Outcomes Without Covariates
Before covariate adjustment, prenatal cannabis exposure only before and after maternal knowledge of pregnancy were associated with higher PLEs, BMI, and internalizing, externalizing, attention, thought, social, and sleep problems, as well as lower cognition and GMV, relative to no prenatal exposure (all |β| > 0.02; all FDR-corrected P < .03; Table 2). Prenatal exposure after, but not before, maternal knowledge of pregnancy was also associated with lower birth weight, ICV, and WMV when compared with those with no prenatal exposure (all |β| > 0.07; all FDR-corrected P < .002; Table 2). Comparing groups with prenatal exposure revealed that exposure after maternal knowledge of pregnancy was associated with relatively higher psychopathology across all measures, BMI, sleep problems, lower cognition, birth weight, ICV, GMV, and WMV (all |β| > 0.02; all FDR-corrected P < .05; Table 2). Prenatal cannabis exposure explained less than 1.9% of the variance in outcomes.
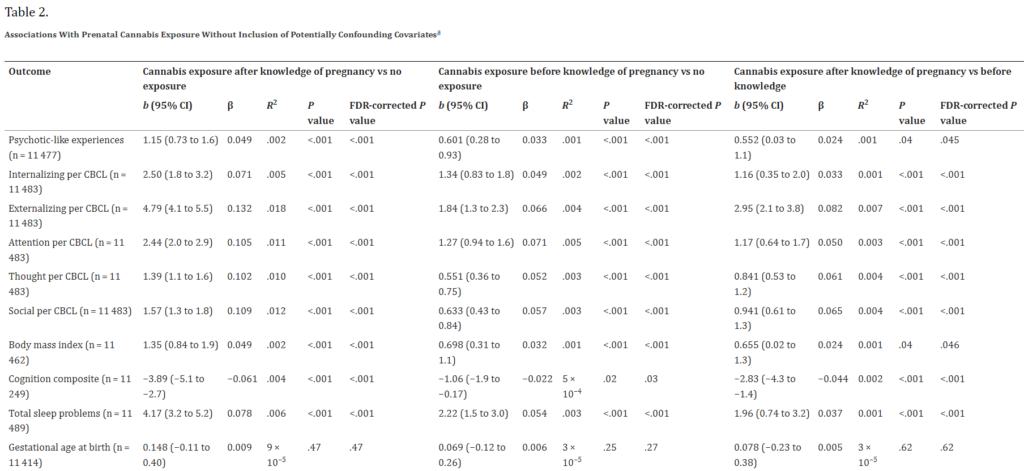

Abbreviations: CBCL, Child Behavior Checklist; FDR, false discovery rate.
aLinear mixed-effect models were used to analyze the associations between prenatal cannabis exposure (a factor variable with 3 mutually exclusive groups: no exposure, exposure before maternal knowledge of pregnancy, and exposure after maternal knowledge of pregnancy) and each outcome, nesting data by research site and family identification (nonimaging analyses) and scanner and family identification (imaging analyses). Psychotic-like experiences were assessed with the Prodromal Questionnaire Brief–Report Child Version, uncorrected cognition composite from the National Institutes of Health Toolbox, and sleep problems from the Parent Sleep Disturbance Scale for Children. Numbers differ owing to listwise deletion of missing data. The b values are unstandardized; β coefficients are standardized. P values after FDR correction for multiple testing, calculated separately for cannabis exposure before maternal knowledge of pregnancy and cannabis exposure after maternal knowledge of pregnancy.
Association of Prenatal Cannabis Exposure and Outcomes With Covariates
When including covariates, exposure after knowledge of pregnancy remained associated with higher PLEs as well as externalizing, attention, thought, and social problems relative to those with no reported prenatal exposure and those with exposure only before maternal knowledge of pregnancy (all |β| > 0.02; all FDR-corrected P < .02; Figure and Table 3; eTables 1-7 in the Supplement). These associations explained less than 0.4% of variance in outcomes. Full regression results are provided in eTables 1, 2, and 3 in the Supplement. While they did not survive FDR correction, exposure after maternal knowledge was also associated with greater internalizing problems and reduced birth weight relative to both other groups at nominal/marginal levels of significance (all |β| > 0.02; all P < .064; all FDR-corrected P < .12) as well as reduced cognition relative to exposure only before maternal knowledge (β = −0.023; P = .043; FDR-corrected P = .07; Figure and Table 3). Of note, effect sizes (ie, β coefficients) for group differences when comparing prenatal cannabis exposure after knowledge with either no exposure or exposure only before knowledge of pregnancy were roughly equivalent (Table 3). No group differences were found when comparing prenatal cannabis exposure before maternal knowledge of pregnancy with no exposure. Generally, no small group of covariates was responsible for attenuating these associations (eResults in the Supplement).
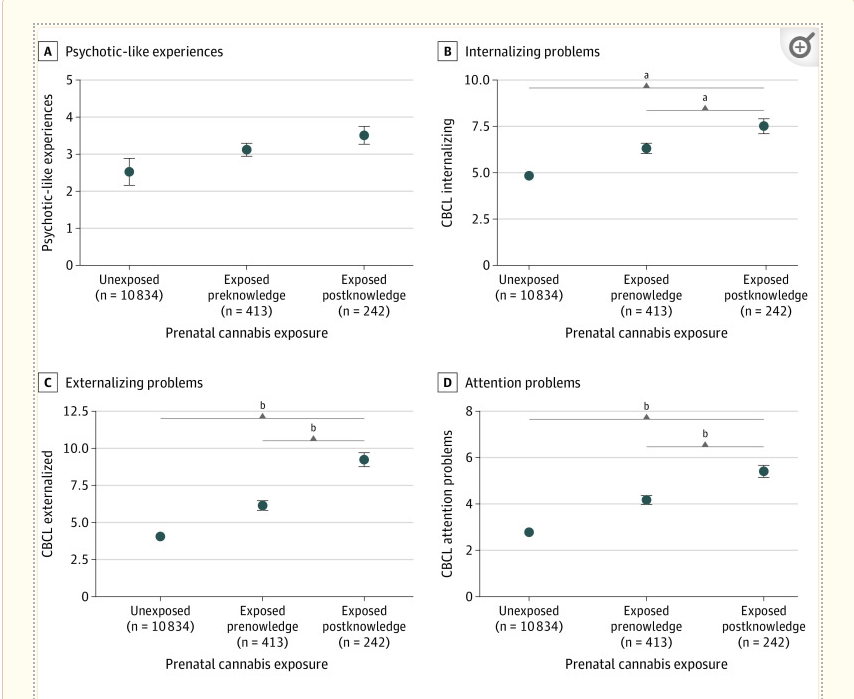
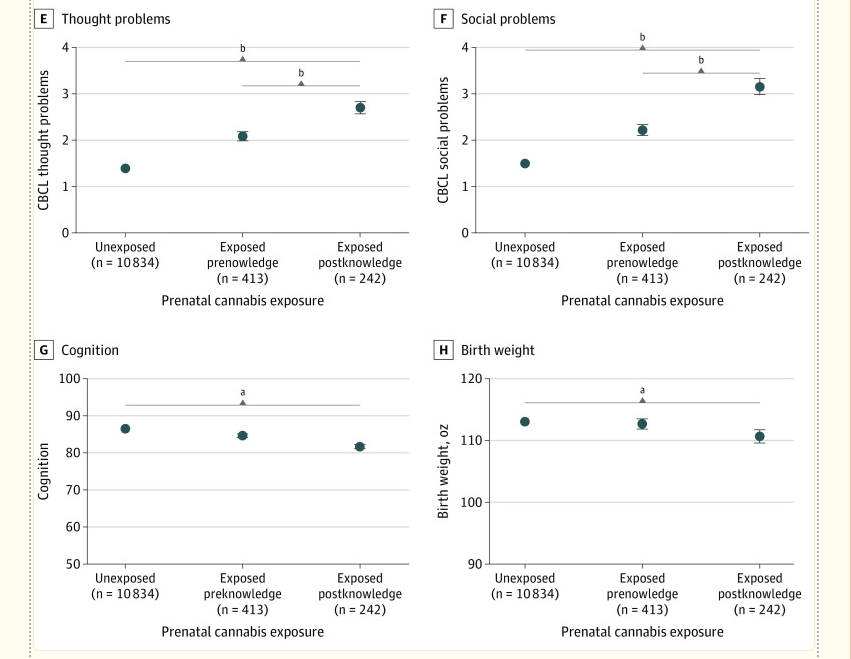
Association of Prenatal Cannabis Exposure After Maternal Knowledge of Pregnancy With Risk of Adverse Childhood Outcomes
A, Psychotic-like experiences. B, Internalizing problems. C, Externalizing problems. D, Attention problems. E, Thought problems. F, Social problems. G, Cognition. H, Birth weight. Raw data values are plotted. As scales differ, y axes are not directly comparable across panels. Vertical lines indicate SEs. Statistics are presented in Table 2 and Table 3 and eTables 1 and 2 in the Supplement. Log-transforming data reduce differences in variability across groups and results in similar conclusions (eTable 4 in the Supplement). CBCL indicates Child Behavior Checklist.aP < .05 only before false discovery rate correction.bFalse discovery rate–corrected P < .05.
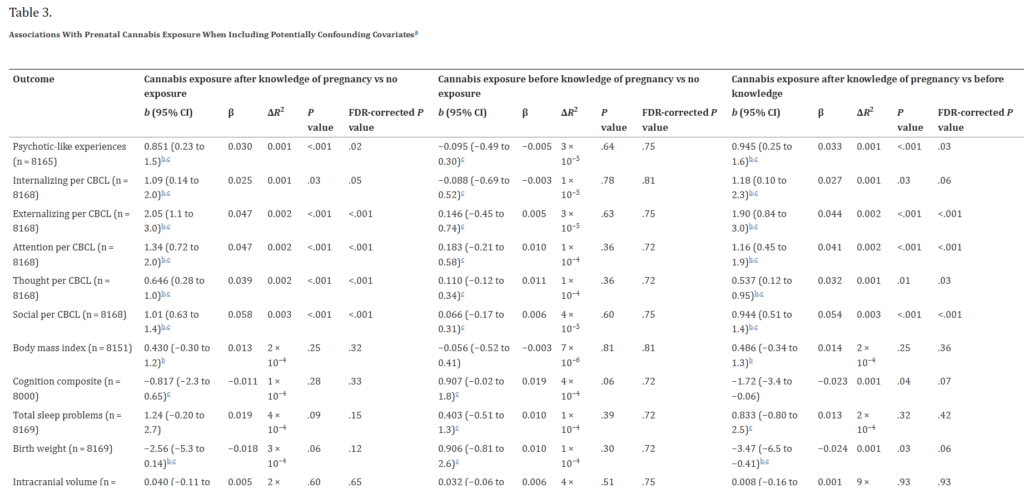

Abbreviations: CBCL, Child Behavior Checklist; FDR, false discovery rate. aSee Methods. Numbers differ owing to listwise deletion. The b values are unstandardized; β coefficients are standardized. bWald tests of the equality of coefficients revealed that β estimates did not differ between the following contrasts: after knowledge exposure vs no exposure and after knowledge exposure vs before knowledge exposure (χ2 < 0.64; P > .26). cWald tests of the equality of coefficients revealed that β estimates did differ between the following contrasts: after knowledge exposure vs no exposure and before knowledge exposure vs no exposure, as well as before knowledge exposure vs no exposure and after knowledge exposure vs before knowledge exposure (χ2 > 2.09; P < .05).
Post hoc analyses excluding children who engaged in uncommon substance use, who were exposed to other illicit substances prenatally, who were born at extreme levels of prematurity (eMethods in the Supplement), or whose biological mothers were not the parent or caregiver respondent revealed consistent findings (eTables 9-12 in the Supplement). Log-transforming outcomes or including only covariates significantly associated with outcomes in the full regression models did not meaningfully alter any observed associations (eTables 4-7 and 12 in the Supplement). Five-fold cross-validation suggests that inclusion of all covariates did not appreciably alter the stability of β coefficient estimates. This finding suggests that our primary analytic approach did not alter β estimates by overfitting these data (eMethods and eTable 8 in the Supplement). Finally, in the subsample of children with genomically confirmed European ancestry (181 of 4591 [3.9%] reporting any prenatal exposure), PLEs and social problems remained more associated with exposure after maternal knowledge of pregnancy. Further accounting for child PGS for schizophrenia, educational level, and/or cannabis use did not substantively alter the findings (eTables 13-16 in the Supplement).
Sensitivity Analyses
As prenatal exposure after maternal knowledge, regardless of contrast group (ie, no exposure or exposure only before maternal knowledge), was associated with outcomes (Table 3), we conducted regression analyses with prenatal exposure coded as 2 nonmutually exclusive exposure variables (ie, any exposure before or after knowledge) and the results remained unchanged. To account for possible imbalance in covariate distributions across exposed and unexposed individuals, we also conducted inverse probability propensity score–weighted analyses, which also broadly recapitulated the conclusions reported above (eTables 17-20 in the Supplement).
Discussion
This study suggests that prenatal cannabis exposure after maternal knowledge of pregnancy is associated with a small elevation in risk for psychopathology during childhood (Table 2 and Table 3). That these associations were robust to the inclusion of potentially confounding variables increases the plausibility that prenatal cannabis exposure may be independently associated with psychopathology risk in children. In contrast to increasingly permissive attitudes surrounding cannabis use among pregnant mothers45 and suggestions by dispensaries to use cannabis to combat pregnancy-related nausea,46 our findings align with recent recommendations by the US Surgeon General14 regarding the potential association of in utero cannabis exposure with outcomes in children.
All studied outcomes except gestational age at birth were associated with prenatal exposure before and after maternal knowledge of pregnancy relative to no exposure; however, only associations between prenatal exposure after maternal knowledge of pregnancy and child psychopathology were robust to covariate inclusion, with birth weight and sleep problems showing nonsignificant nominal trends (Table 3). Effect size estimates were largely overlapping when contrasting prenatal exposure after maternal knowledge of pregnancy vs no prenatal exposure and vs prenatal exposure before maternal knowledge of pregnancy (Table 3); regression analyses of prenatal exposure after knowledge of pregnancy vs no exposure after knowledge (ie, no exposure and exposure only before maternal knowledge of pregnancy) produced equivalent findings (eTable 18 in the Supplement). Collectively, these findings suggest that prenatal exposure after maternal knowledge of pregnancy may plausibly be independently associated with child outcomes, while associations with exposure only before maternal knowledge of pregnancy may be attributable to confounding variables, such as familial and pregnancy-related factors correlated with cannabis use and/or offspring outcomes.
There are several potential explanations for the overall pattern of findings. First, endocannabinoid system ontogeny may play a role. Animal models suggest that endocannabinoid type 1 receptors (CB1Rs) are critical for THC’s impact on the developing brain47 and are not expressed before the equivalent of 5 to 6 weeks’ gestation in humans.9 Independent associations of cannabis with child behavioral outcomes may arise only when sufficient CB1Rs are present in the fetus, which may not occur until many women learn they are pregnant. It is possible that exposure before this time might not have a direct association with fetal brain development, although it remains possible that there may be indirect associations through endocannabinoid receptor expression in the placenta.48 Excluding women who reported only using cannabis prior to knowledge of pregnancy but learning of their pregnancy at more than 14 weeks’ or more than 9 weeks’ gestation produced consistent results (eTables 21 and 22 in the Supplement). Second, use of cannabis despite knowledge of pregnancy might represent a preexisting and more severe form of cannabis use (eg, cannabis use disorder), indicative of greater prenatal and potential postnatal exposure (eg, through breastfeeding).49 Third, sustained cannabis use during pregnancy may reflect a predisposition to the observed negative outcomes (eg, socioeconomic status and genetic susceptibility).50,51 However, controlling for such factors did not eliminate associations (eTables 2, 3, 13, and 14 in the Supplement). Fourth, associations may be attributable to an unmeasured common variable (eg, paternal germline exposure to cannabis, health care access, or postpartum maternal behavior)52,53 or an alternative derivation of an included confounder. Accounting for scores from a 4-item assessment of PLEs in mothers (eMethods in the Supplement) as opposed to familial history of psychosis, which has a low rate of report, does not alter the significance of the association between prenatal cannabis exposure and PLEs in offspring (eTable 23 in the Supplement).
Chronic self-administration of cannabis during adolescence has been linked to increased psychopathology, particularly psychosis.54 In contrast to acute THC psychotomimetic effects,55 mounting evidence supports common genetic liability as a major factor in this association,44,51,56,57,58 although potential bidirectional44,51,59,60,61 causal effects cannot be ruled out. Consistent with prior work,21 we find that child psychosis liability (ie, PLEs and thought problems) is modestly higher among children prenatally exposed to cannabis after maternal knowledge of pregnancy. That the association with PLEs remained after accounting for family history of psychosis as well as child PGS suggests that this association may not be entirely attributable to common genomic liability, as indexed by PGS and family history. Putative mechanisms underlying psychosis liability in children prenatally exposed to cannabis may be distinct from those associated with self-administered cannabis use. For instance, CB1Rs have neuromodulatory functions throughout life, but during the prenatal period they are ubiquitously expressed in neural progenitors and contribute to neural migration, axonal elongation, and synaptic formation.9 Although abnormalities in these neural processes are consistent with neurodevelopmental theories of psychosis,62 the associations we observed with metrics of gross brain morphologic characteristics were not robust to covariate inclusion. It is possible that neurodevelopmental differences (eg, synaptic formation) are not detectable using magnetic resonance imaging, are regionally specific, or emerge at different developmental stages.
In addition to associations with PLEs and thought problems, children prenatally exposed to cannabis after maternal knowledge of pregnancy had elevated externalizing, attention, and social problems. Prenatal exposure to alcohol and tobacco were also associated with psychopathology in offspring, but these associations were predominantly with exposure prior to, as opposed to after, maternal knowledge of pregnancy and were observed inconsistently relative to associations with cannabis exposure (eTables 1 and 2 in the Supplement). The lack of association with alcohol or tobacco use subsequent to knowledge of pregnancy may indicate the more pronounced public awareness of fetal risks and obstetric oversight of the use of these substances that is associated with greater reductions in use after knowledge of pregnancy, relative to cannabis,8,63 as well as phenotypic heterogeneity encompassed by our dichotomous phenotypes. Alternatively, prenatal cannabis exposure may serve as a proxy for exposure to a permissive home environment that promotes externalizing behaviors and related cognitive disengagement.64 As has been shown for the increased likelihood of tobacco smoking during pregnancy in women with attention-deficit/hyperactivity disorder and the confounding of consequent associations with attention-deficit/hyperactivity disorder in offspring,65,66,67 women with externalizing features might be more likely to continue using cannabis during their pregnancy. Although our consideration of covariates suggests potential independent associations of cannabis with these outcomes, genetically informed designs (eg, sibling crossover design where nontwin siblings are discordant for prenatal exposure)68,69 would be a useful approach to consider familial sources of confounding.70
Limitations
Some limitations of this study are noteworthy. First, parents or caregivers retrospectively reported on cannabis use during pregnancy that occurred approximately 10 years earlier, which may have resulted in biased reporting and misclassification.71 For example, retrospective report of substance use during pregnancy 14 years earlier has been found to be more common than antenatal report and more strongly correlated with child outcomes (eg, measured birth weight and behavioral problems).71 Although these findings may indicate greater accuracy during retrospective recall, they could also reflect recall bias related to children contemporaneously experiencing problems. However, ABCD Study prevalence estimates of self-reported prenatal cannabis use align with toxicology-based prevalence estimates from national data sets collected during the years these children were born.72
Second, although the ABCD Study is, to our knowledge, the largest integrative study of child health and substance use and among the largest studies of prenatal exposure and child outcomes (the number of exposed children exceeded entire samples from other studies),21 there was a proportionally small number of participants who were exposed to cannabis prenatally, thereby reducing power. Third, THC concentration differs between fetuses whose mothers use cannabis once per month compared with once per day.15 There are limited or no data on potency, frequency (see Results), timing, or quantity of cannabis exposure in this data set. It will be important for future efforts to better understand the impact of dosage, strain, and method of ingestion.73 Fourth, while we were able to account for many known familial, pregnancy-related, and child-related confounding variables, the role of unmeasured confounders cannot be discounted. Relatedly, while we account for underlying genetic vulnerability using both familial history and PGS, it is possible that the current genome-wide association studies from which PGS weighting was estimated do not adequately represent genetic risk for the specific child outcomes under study (eTables 15 and 16 in the Supplement).
Conclusions
Despite increasingly permissive social attitudes and the marked relaxation of legal restrictions on cannabis use,1 prenatal cannabis exposure and the correlated risks that it indexes may place offspring at increased risk for psychopathology in middle childhood. In the context of increasing cannabis use among pregnant women,2,6 it is clear that more studies on the association between prenatal cannabis exposure and offspring developmental outcomes are needed to examine potential causal effects, moderating or protective factors, and biological mechanisms.74,75 Similar to the effective messaging surrounding the adverse consequences of alcohol and tobacco exposure during pregnancy, education regarding the potential harms associated with prenatal cannabis use is necessary. Currently, pregnant women, and even those contemplating pregnancy, should be discouraged from using any cannabis by health care professionals, dispensaries, and others; women refraining from cannabis use during pregnancy may benefit offspring.11,14
Notes
Supplement.
eMethods.
eResults.
eTable 1. Full Regression Results From Models Examining Associations Between Prenatal Cannabis Exposure and CBCL Outcomes When Including Potentially Confounding Covariates
eTable 2. Full Regression Results From Models Examining Associations Between Prenatal Cannabis Exposure and Psychotic-Like Experiences, BMI, Cognition, Sleep Problems, and Birth Weight When Including Potentially Confounding Covariates
eTable 3. Full Regression Results From Models Examining Associations Between Prenatal Cannabis Exposure and Brain Structure Metrics When Including Potentially Confounding Covariates
eTable 4. Regression Results From Models Examining Associations Between Prenatal Cannabis Exposure and Log-Transformed Outcomes When Including Potentially Confounding Covariates
eTable 5. Full Regression Results From Models Examining Associations Between Prenatal Cannabis Exposure and CBCL Outcomes When Including Potentially Confounding Covariates Associated With the Outcome Only
eTable 6. Psychotic-Like Experiences, BMI, Cognition, Sleep, and Birth Weight Models With Significant Fixed Effect Covariates Only
eTable 7. Brain Structure Models With Significant Fixed Effect Covariates Only
eTable 8. Test of Overfitting Results From 5-Fold Cross Validation
eTable 9. Regression Results When Excluding Children With Non-Prevalent Substance Use
eTable 10. Regression Results When Excluding Children Prenatally Exposed to Illicit Substances Other Than Marijuana
eTable 11. Regression Results When Excluding Children Born at Extreme Prematurity
eTable 12. Regression Results When Excluding Children Who Had a Non-Biological Mother Report as the Parent/Caregiver Respondent
eTable 13. Regression Results Restricted to the Subsample of Individuals With Genomically-Confirmed European Ancestry
eTable 14. Regression Results When Including Polygenic Risk Scores and Ancestrally-Informative Principal Components as Additional Covariates
eTable 15. Associations Between Psychotic-Like Experiences and Polygenic Scores for Schizophrenia, Educational Attainment, and Cannabis Use
eTable 16. Associations Between Social Problems and Polygenic Scores for Cannabis Use
eTable 17. Non-Mutually Exclusive Groups Regression Results Without Covariates
eTable 18. Non-Mutually Exclusive Groups Regression Results With Covariates
eTable 19. Inverse Probability Weighting Balance Analysis Results
eTable 20. Inverse Probability Weighting Regression Results
eTable 21. Regression Results When Excluding Children Whose Mother Used Cannabis Only Prior to Pregnancy Knowledge and Discovered Pregnancy After 15 Weeks
eTable 22. Regression Results When Excluding Children Whose Mother Used Cannabis Only Prior to Pregnancy Knowledge and Discovered Pregnancy After 9 Weeks
eTable 23. Psychotic-Like Experiences and Prenatal Cannabis Exposure: Regression Results When Including Maternal Psychotic-Like Experiences as a Covariate
Click here for additional data file.(901K, pdf)
References
1. Hasin DS. US epidemiology of cannabis use and associated problems. Neuropsychopharmacology. 2018;43(1):195-212. doi: 10.1038/npp.2017.198 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
2. Volkow ND, Han B, Compton WM, McCance-Katz EF. Self-reported medical and nonmedical cannabis use among pregnant women in the United States. JAMA. 2019;322(2):167-169. doi: 10.1001/jama.2019.7982 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
3. Yao JL, He QZ, Liu M, et al.. Effects of Δ(9)-tetrahydrocannabinol (THC) on human amniotic epithelial cell proliferation and migration. Toxicology. 2018;394:19-26. doi: 10.1016/j.tox.2017.11.016 [PubMed] [CrossRef] [Google Scholar]
4. Basavarajappa BS, Nixon RA, Arancio O. Endocannabinoid system: emerging role from neurodevelopment to neurodegeneration. Mini Rev Med Chem. 2009;9(4):448-462. doi: 10.2174/138955709787847921 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
5. Fride E, Gobshtis N, Dahan H, Weller A, Giuffrida A, Ben-Shabat S. The endocannabinoid system during development: emphasis on perinatal events and delayed effects. Vitam Horm. 2009;81:139-158. doi: 10.1016/S0083-6729(09)81006-6 [PubMed] [CrossRef] [Google Scholar]
6. Young-Wolff KC, Sarovar V, Tucker LY, et al.. Self-reported daily, weekly, and monthly cannabis use among women before and during pregnancy. JAMA Netw Open. 2019;2(7):e196471. doi: 10.1001/jamanetworkopen.2019.6471 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
7. Brown QL, Sarvet AL, Shmulewitz D, Martins SS, Wall MM, Hasin DS. Trends in marijuana use among pregnant and nonpregnant reproductive-aged women, 2002-2014. JAMA. 2017;317(2):207-209. doi: 10.1001/jama.2016.17383 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
8. Agrawal A, Rogers CE, Lessov-Schlaggar CN, Carter EB, Lenze SN, Grucza RA. Alcohol, cigarette, and cannabis use between 2002 and 2016 in pregnant women from a nationally representative sample. JAMA Pediatr. 2019;173(1):95-96. doi: 10.1001/jamapediatrics.2018.3096 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
9. Wu CS, Jew CP, Lu HC. Lasting impacts of prenatal cannabis exposure and the role of endogenous cannabinoids in the developing brain. Future Neurol. 2011;6(4):459-480. doi: 10.2217/fnl.11.27 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10. Scheyer AF, Melis M, Trezza V, Manzoni OJJ. Consequences of perinatal cannabis exposure. Trends Neurosci. 2019;42(12):871-884. doi: 10.1016/j.tins.2019.08.010 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
11. Volkow ND, Compton WM, Wargo EM. The risks of marijuana use during pregnancy. JAMA. 2017;317(2):129-130. doi: 10.1001/jama.2016.18612 [PubMed] [CrossRef] [Google Scholar]
12. Jansson LM, Jordan CJ, Velez ML. Perinatal marijuana use and the developing child. JAMA. 2018;320(6):545-546. doi: 10.1001/jama.2018.8401 [PubMed] [CrossRef] [Google Scholar]
13. National Academies of Sciences, Engineering, and Medicine The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. National Academies Press; 2017. [Google Scholar]
14. Office of the Surgeon General, US Department of Health and Human Services. U.S. Surgeon General’s advisory: marijuana use and the developing brain. Accessed October 16, 2019. https://www.hhs.gov/surgeongeneral/reports-and-publications/addiction-and-substance-misuse/advisory-on-marijuana-use-and-developing-brain/index.html#
15. Ryan SA, Ammerman SD, O’Connor ME; Committee on Substance Use and Prevention; Section on Breastfeeding . Marijuana use during pregnancy and breastfeeding: implications for neonatal and childhood outcomes. Pediatrics. 2018;142(3):e20181889. doi: 10.1542/peds.2018-1889 [PubMed] [CrossRef] [Google Scholar]
16. Smith AM, Mioduszewski O, Hatchard T, Byron-Alhassan A, Fall C, Fried PA. Prenatal marijuana exposure impacts executive functioning into young adulthood: an fMRI study. Neurotoxicol Teratol. 2016;58:53-59. doi: 10.1016/j.ntt.2016.05.010 [PubMed] [CrossRef] [Google Scholar]
17. Leech SL, Richardson GA, Goldschmidt L, Day NL. Prenatal substance exposure: effects on attention and impulsivity of 6-year-olds. Neurotoxicol Teratol. 1999;21(2):109-118. doi: 10.1016/S0892-0362(98)00042-7 [PubMed] [CrossRef] [Google Scholar]
18. Corsi DJ, Walsh L, Weiss D, et al.. Association between self-reported prenatal cannabis use and maternal, perinatal, and neonatal outcomes. JAMA. 2019;322(2):145-152. doi: 10.1001/jama.2019.8734 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
19. Gray KA, Day NL, Leech S, Richardson GA. Prenatal marijuana exposure: effect on child depressive symptoms at ten years of age. Neurotoxicol Teratol. 2005;27(3):439-448. doi: 10.1016/j.ntt.2005.03.010 [PubMed] [CrossRef] [Google Scholar]
20. Goldschmidt L, Day NL, Richardson GA. Effects of prenatal marijuana exposure on child behavior problems at age 10. Neurotoxicol Teratol. 2000;22(3):325-336. doi: 10.1016/S0892-0362(00)00066-0 [PubMed] [CrossRef] [Google Scholar]
21. Day NL, Goldschmidt L, Day R, Larkby C, Richardson GA. Prenatal marijuana exposure, age of marijuana initiation, and the development of psychotic symptoms in young adults. Psychol Med. 2015;45(8):1779-1787. doi: 10.1017/S0033291714002906 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
22. Dahl RE, Scher MS, Williamson DE, Robles N, Day N. A longitudinal study of prenatal marijuana use: effects on sleep and arousal at age 3 years. Arch Pediatr Adolesc Med. 1995;149(2):145-150. doi: 10.1001/archpedi.1995.02170140027004 [PubMed] [CrossRef] [Google Scholar]
23. Zammit S, Thomas K, Thompson A, et al.. Maternal tobacco, cannabis and alcohol use during pregnancy and risk of adolescent psychotic symptoms in offspring. Br J Psychiatry. 2009;195(4):294-300. doi: 10.1192/bjp.bp.108.062471 [PubMed] [CrossRef] [Google Scholar]
24. Ruisch IH, Dietrich A, Glennon JC, Buitelaar JK, Hoekstra PJ. Maternal substance use during pregnancy and offspring conduct problems: a meta-analysis. Neurosci Biobehav Rev. 2018;84:325-336. doi: 10.1016/j.neubiorev.2017.08.014 [PubMed] [CrossRef] [Google Scholar]
25. Huizink AC. Prenatal cannabis exposure and infant outcomes: overview of studies. Prog Neuropsychopharmacol Biol Psychiatry. 2014;52:45-52. doi: 10.1016/j.pnpbp.2013.09.014 [PubMed] [CrossRef] [Google Scholar]
26. Fine JD, Moreau AL, Karcher NR, et al.. Association of Prenatal cannabis exposure with psychosis proneness among children in the Adolescent Brain Cognitive Development (ABCD) Study. JAMA Psychiatry. 2019;76(7):762-764. doi: 10.1001/jamapsychiatry.2019.0076 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
27. Buckley NE, Hansson S, Harta G, Mezey E. Expression of the CB1 and CB2 receptor messenger RNAs during embryonic development in the rat. Neuroscience. 1998;82(4):1131-1149. doi: 10.1016/S0306-4522(97)00348-5 [PubMed] [CrossRef] [Google Scholar]
28. Zurolo E, Iyer AM, Spliet WG, et al.. CB1 and CB2 cannabinoid receptor expression during development and in epileptogenic developmental pathologies. Neuroscience. 2010;170(1):28-41. doi: 10.1016/j.neuroscience.2010.07.004 [PubMed] [CrossRef] [Google Scholar]
29. Volkow ND, Koob GF, Croyle RT, et al.. The conception of the ABCD Study: from substance use to a broad NIH collaboration. Dev Cogn Neurosci. 2018;32:4-7. doi: 10.1016/j.dcn.2017.10.002 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
30. Karcher NR, Barch DM, Avenevoli S, et al.. Assessment of the Prodromal Questionnaire–Brief Child Version for measurement of self-reported psychoticlike experiences in childhood. JAMA Psychiatry. 2018;75(8):853-861. doi: 10.1001/jamapsychiatry.2018.1334 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
31. Loewy RL, Pearson R, Vinogradov S, Bearden CE, Cannon TD. Psychosis risk screening with the Prodromal Questionnaire–Brief Version (PQ-B). Schizophr Res. 2011;129(1):42-46. doi: 10.1016/j.schres.2011.03.029 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
32. Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles: An Integrated System of Multi-informant Assessment. ASEBA; 2001. [Google Scholar]
33. Akshoomoff N, Beaumont JL, Bauer PJ, et al.. VIII. NIH Toolbox Cognition Battery (CB): composite scores of crystallized, fluid, and overall cognition. Monogr Soc Res Child Dev. 2013;78(4):119-132. doi: 10.1111/mono.12038 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
34. Bruni O, Ottaviano S, Guidetti V, et al.. The Sleep Disturbance Scale for Children (SDSC): construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. 1996;5(4):251-261. doi: 10.1111/j.1365-2869.1996.00251.x [PubMed] [CrossRef] [Google Scholar]
35. FreeSurfer FreeSurfer software suite. Accessed August 12, 2020. http://surfer.nmr.mgh.harvard.edu/
36. Dale AM, Fischl B, Sereno MI. Cortical surface–based analysis, I: segmentation and surface reconstruction. Neuroimage. 1999;9(2):179-194. doi: 10.1006/nimg.1998.0395 [PubMed] [CrossRef] [Google Scholar]
37. Fischl B, van der Kouwe A, Destrieux C, et al.. Automatically parcellating the human cerebral cortex. Cereb Cortex. 2004;14(1):11-22. doi: 10.1093/cercor/bhg087 [PubMed] [CrossRef] [Google Scholar]
38. Casey BJ, Cannonier T, Conley MI, et al.; ABCD Imaging Acquisition Workgroup . The Adolescent Brain Cognitive Development (ABCD) Study: imaging acquisition across 21 sites. Dev Cogn Neurosci. 2018;32:43-54. doi: 10.1016/j.dcn.2018.03.001 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
39. Hagler DJ Jr, Hatton S, Cornejo MD, et al.. Image processing and analysis methods for the Adolescent Brain Cognitive Development Study. Neuroimage. 2019;202:116091. doi: 10.1016/j.neuroimage.2019.116091 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
40. Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Software. 2015;67(1):48. doi: 10.18637/jss.v067.i01 [CrossRef] [Google Scholar]
41. Bogdan R, Baranger DAA, Agrawal A. Polygenic risk scores in clinical psychology: bridging genomic risk to individual differences. Annu Rev Clin Psychol. 2018;14:119-157. doi: 10.1146/annurev-clinpsy-050817-084847 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
42. Schizophrenia Working Group of the Psychiatric Genomics Consortium Biological insights from 108 schizophrenia-associated genetic loci. Nature. 2014;511(7510):421-427. doi: 10.1038/nature13595 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
43. Lee JJ, Wedow R, Okbay A, et al.; 23andMe Research Team; COGENT (Cognitive Genomics Consortium); Social Science Genetic Association Consortium . Gene discovery and polygenic prediction from a genome-wide association study of educational attainment in 1.1 million individuals. Nat Genet. 2018;50(8):1112-1121. doi: 10.1038/s41588-018-0147-3 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
44. Pasman JA, Verweij KJH, Gerring Z, et al.; 23andMe Research Team; Substance Use Disorders Working Group of the Psychiatric Genomics Consortium; International Cannabis Consortium . GWAS of lifetime cannabis use reveals new risk loci, genetic overlap with psychiatric traits, and a causal influence of schizophrenia. Nat Neurosci. 2018;21(9):1161-1170. doi: 10.1038/s41593-018-0206-1 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
45. Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the U.S.: a review. Prev Med. 2017;104:13-23. doi: 10.1016/j.ypmed.2017.07.008 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
46. Dickson B, Mansfield C, Guiahi M, et al.. Recommendations from cannabis dispensaries about first-trimester cannabis use. Obstet Gynecol. 2018;131(6):1031-1038. doi: 10.1097/AOG.0000000000002619 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
47. de Salas-Quiroga A, Díaz-Alonso J, García-Rincón D, et al.. Prenatal exposure to cannabinoids evokes long-lasting functional alterations by targeting CB1 receptors on developing cortical neurons. Proc Natl Acad Sci U S A. 2015;112(44):13693-13698. doi: 10.1073/pnas.1514962112 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
48. Fügedi G, Molnár M, Rigó J Jr, Schönléber J, Kovalszky I, Molvarec A. Increased placental expression of cannabinoid receptor 1 in preeclampsia: an observational study. BMC Pregnancy Childbirth. 2014;14:395. doi: 10.1186/s12884-014-0395-x [PMC free article] [PubMed] [CrossRef] [Google Scholar]
49. Baranger DAA, Bogdan R. Editorial: causal, predispositional, or correlate? group differences in cognitive control–related brain function in cannabis-using youth raise new questions. J Am Acad Child Adolesc Psychiatry. 2019;58(7):665-667. doi: 10.1016/j.jaac.2019.05.018 [PubMed] [CrossRef] [Google Scholar]
50. Baranger DAA, Demers CH, Elsayed NM, et al.. Convergent evidence for predispositional effects of brain gray matter volume on alcohol consumption. Biol Psychiatry. 2020;87(7):645-655. doi: 10.1016/j.biopsych.2019.08.029 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
51. Demontis D, Rajagopal VM, Thorgeirsson TE, et al.. Genome-wide association study implicates CHRNA2 in cannabis use disorder. Nat Neurosci. 2019;22(7):1066-1074. doi: 10.1038/s41593-019-0416-1 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
52. Murphy SK, Itchon-Ramos N, Visco Z, et al.. Cannabinoid exposure and altered DNA methylation in rat and human sperm. Epigenetics. 2018;13(12):1208-1221. doi: 10.1080/15592294.2018.1554521 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
53. Bishai R, Koren G. Maternal and obstetric effects of prenatal drug exposure. Clin Perinatol. 1999;26(1):75-86, vii. doi: 10.1016/S0095-5108(18)30073-3 [PubMed] [CrossRef] [Google Scholar]
54. Moore TH, Zammit S, Lingford-Hughes A, et al.. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328. doi: 10.1016/S0140-6736(07)61162-3 [PubMed] [CrossRef] [Google Scholar]
55. Mason O, Morgan CJ, Dhiman SK, et al.. Acute cannabis use causes increased psychotomimetic experiences in individuals prone to psychosis. Psychol Med. 2009;39(6):951-956. doi: 10.1017/S0033291708004741 [PubMed] [CrossRef] [Google Scholar]
56. Power RA, Verweij KJ, Zuhair M, et al.. Genetic predisposition to schizophrenia associated with increased use of cannabis. Mol Psychiatry. 2014;19(11):1201-1204. doi: 10.1038/mp.2014.51 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
57. Carey CE, Agrawal A, Bucholz KK, et al.. Associations between polygenic risk for psychiatric disorders and substance involvement. Front Genet. 2016;7:149. doi: 10.3389/fgene.2016.00149 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
58. Verweij KJ, Abdellaoui A, Nivard MG, et al.; International Cannabis Consortium . Short communication: genetic association between schizophrenia and cannabis use. Drug Alcohol Depend. 2017;171:117-121. doi: 10.1016/j.drugalcdep.2016.09.022 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
59. Vaucher J, Keating BJ, Lasserre AM, et al.. Cannabis use and risk of schizophrenia: a mendelian randomization study. Mol Psychiatry. 2018;23(5):1287-1292. doi: 10.1038/mp.2016.252 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
60. Karcher NR, Barch DM, Demers CH, et al.. Genetic predisposition vs individual-specific processes in the association between psychotic-like experiences and cannabis use. JAMA Psychiatry. 2019;76(1):87-94. doi: 10.1001/jamapsychiatry.2018.2546 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
61. Gage SH, Jones HJ, Burgess S, et al.. Assessing causality in associations between cannabis use and schizophrenia risk: a two-sample mendelian randomization study. Psychol Med. 2017;47(5):971-980. doi: 10.1017/S0033291716003172 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
62. Owen MJ, O’Donovan MC, Thapar A, Craddock N. Neurodevelopmental hypothesis of schizophrenia. Br J Psychiatry. 2011;198(3):173-175. doi: 10.1192/bjp.bp.110.084384 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
63. Seiler NK. Alcohol and pregnancy: CDC’s health advice and the legal rights of pregnant women. Public Health Rep. 2016;131(4):623-627. doi: 10.1177/0033354916662222 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
64. Hopson MB, Margolis A, Rauh V, Herbstman J. Impact of the home environment on the relationship between prenatal exposure to environmental tobacco smoke and child behavior. Int J Child Health Hum Dev. 2016;9(4):453-464. [PMC free article] [PubMed] [Google Scholar]
65. D’Onofrio BM, Van Hulle CA, Waldman ID, et al.. Smoking during pregnancy and offspring externalizing problems: an exploration of genetic and environmental confounds. Dev Psychopathol. 2008;20(1):139-164. doi: 10.1017/S0954579408000072 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
66. Skoglund C, Chen Q, D’Onofrio BM, Lichtenstein P, Larsson H. Familial confounding of the association between maternal smoking during pregnancy and ADHD in offspring. J Child Psychol Psychiatry. 2014;55(1):61-68. doi: 10.1111/jcpp.12124 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
67. Palmer RH, Bidwell LC, Heath AC, Brick LA, Madden PA, Knopik VS. Effects of maternal smoking during pregnancy on offspring externalizing problems: contextual effects in a sample of female twins. Behav Genet. 2016;46(3):403-415. doi: 10.1007/s10519-016-9779-1 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
68. Knopik VS, Heath AC, Marceau K, et al.. Missouri mothers and their children: a family study of the effects of genetics and the prenatal environment. Twin Res Hum Genet. 2015;18(5):485-496. doi: 10.1017/thg.2015.46 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
69. Quinn PD, Rickert ME, Weibull CE, et al.. Association between maternal smoking during pregnancy and severe mental illness in offspring. JAMA Psychiatry. 2017;74(6):589-596. doi: 10.1001/jamapsychiatry.2017.0456 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
70. D’Onofrio BM, Class QA, Rickert ME, et al.. Translational epidemiologic approaches to understanding the consequences of early-life exposures. Behav Genet. 2016;46(3):315-328. doi: 10.1007/s10519-015-9769-8 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
71. Hannigan JH, Chiodo LM, Sokol RJ, et al.. A 14-year retrospective maternal report of alcohol consumption in pregnancy predicts pregnancy and teen outcomes. Alcohol. 2010;44(7-8):583-594. doi: 10.1016/j.alcohol.2009.03.003 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
72. Garg M, Garrison L, Leeman L, et al.. Validity of self-reported drug use information among pregnant women. Matern Child Health J. 2016;20(1):41-47. doi: 10.1007/s10995-015-1799-6 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
73. Di Forti M, Quattrone D, Freeman TP, et al.; EU-GEI WP2 Group . The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study. Lancet Psychiatry. 2019;6(5):427-436. doi: 10.1016/S2215-0366(19)30048-3 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
74. Frau R, Miczán V, Traccis F, et al.. Prenatal THC exposure produces a hyperdopaminergic phenotype rescued by pregnenolone. Nat Neurosci. 2019;22(12):1975-1985. doi: 10.1038/s41593-019-0512-2 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
75. Dong C, Chen J, Harrington A, Vinod KY, Hegde ML, Hegde VL. Cannabinoid exposure during pregnancy and its impact on immune function. Cell Mol Life Sci. 2019;76(4):729-743. doi: 10.1007/s00018-018-2955-0 [PMC free article] [PubMed] [CrossRef] [Google Scholar]